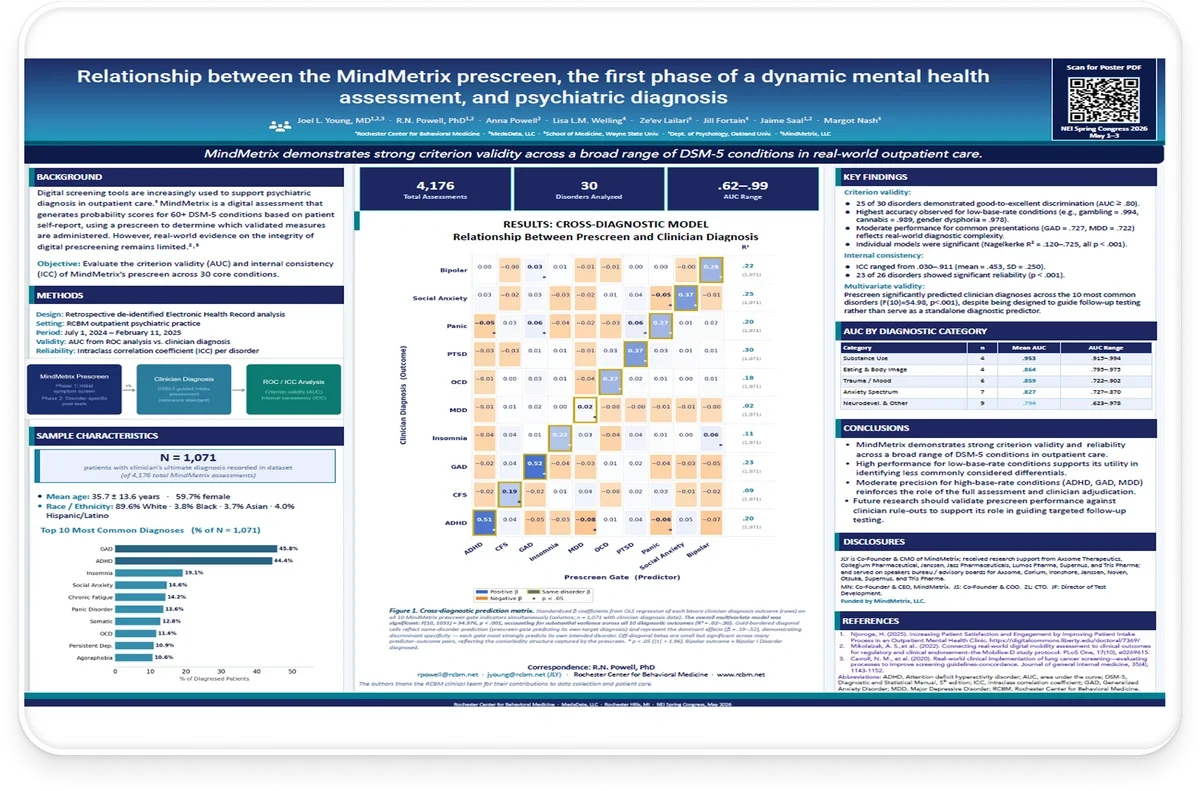
Relationship Between the MindMetrix Prescreen, the First Phase of a Dynamic Mental Health Assessment, and Psychiatric Diagnosis
Presented at NEI Spring 2026
Authors: Joel L. Young, MD; R.N. Powell, PhD; Anna Powell; Lisa L.M. Welling; Ze'ev Lailari; Jill Fortain; Jaime Saal; Margot Nash
Affiliations: Rochester Center for Behavioral Medicine · MedaData, LLC · Rochester Hills, MI
Presented at the NEI Spring Congress, May 1–3, 2026, this research examined the relationship between the MindMetrix prescreen, the first phase of a dynamic mental health assessment, and psychiatric diagnosis. The poster explored whether the prescreen demonstrates criterion validity and reliability across a broad range of DSM-5 conditions in real-world outpatient psychiatric care.
MindMetrix demonstrates strong criterion validity across a broad range of DSM-5 conditions in real-world outpatient care.
Background
Digital screening tools are increasingly used to support psychiatric diagnosis in outpatient care. MindMetrix is a digital assessment that generates probability scores for more than 60 DSM-5 conditions based on patient self-report, using a prescreen to determine which validated measures are administered. However, real-world evidence on the integrity of digital prescreening remains limited.
Objective: Evaluate the criterion validity (AUC) and internal consistency (ICC) of MindMetrix’s prescreen across 30 core conditions.
Methods
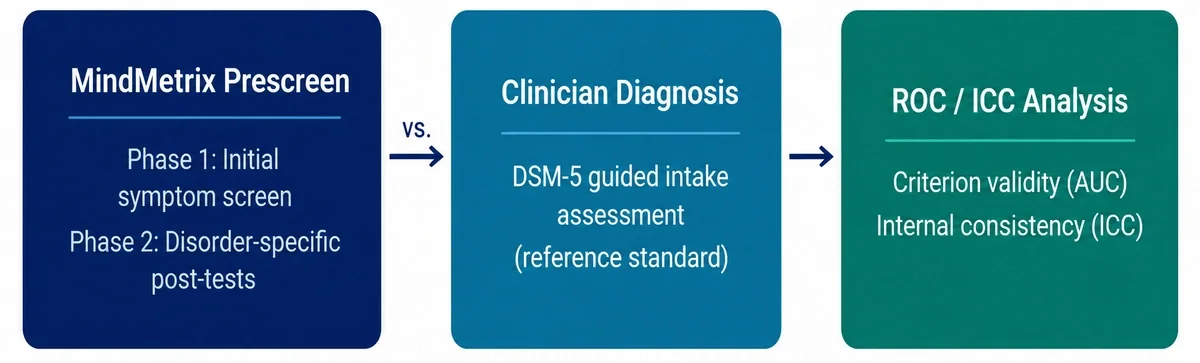
Design
Retrospective de-identified Electronic Health Record analysis.
Setting
RCBM outpatient psychiatric practice
Period
July 1, 2024 – February 11, 2025
Validity
AUC from ROC analysis versus clinician diagnosis.
Reliability
Intraclass correlation coefficient (ICC) per disorder.
Sample Characteristics
The analysis included: 1,071 patients with clinician’s ultimate diagnosis recorded in the dataset, drawn from a total of 4,176 MindMetrix assessments.
Demographics
- Mean age: 35.7 ± 13.6 years
- 59.7% female
- Race / Ethnicity:
- 89.6% White
- 3.8% Black
- 3.7% Asian
- 4.0% Hispanic/Latino
The poster also highlights three key study metrics:
- 4,176 Total Assessments
- 30 Disorders Analyzed
- .62–.99 AUC Range
Top 10 Most Common Diagnoses (% of N = 1,071):
- GAD – 45.8%
- ADHD – 44.4%
- Insomnia – 19.2%
- Social Anxiety – 14.6%
- Chronic Fatigue – 14.2%
- Panic Disorder – 13.6%
- Somatic – 12.8%
- OCD – 11.6%
- Persistent Depression – 10.9%
- Agoraphobia – 10.6%
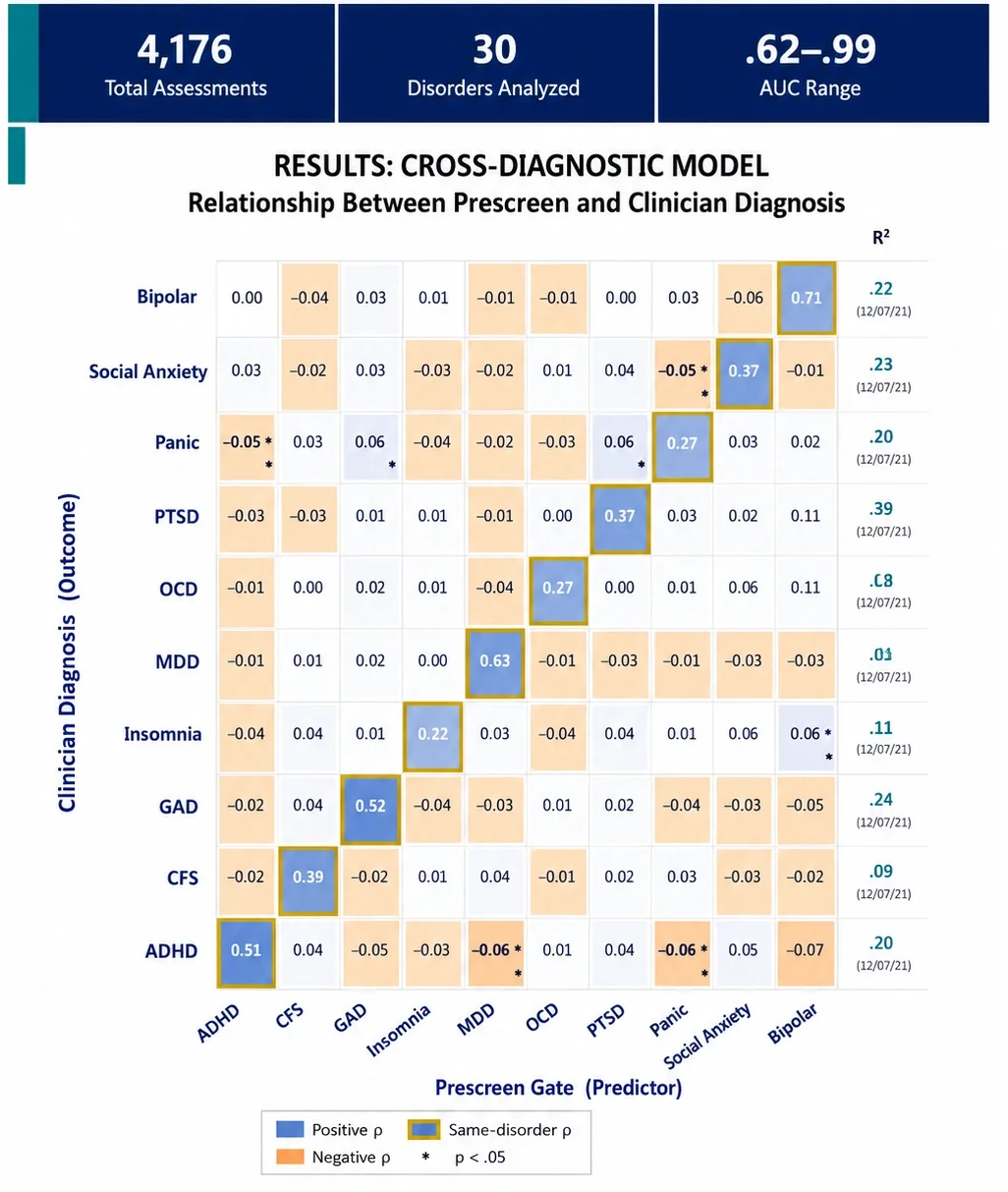
The central analysis examined how each MindMetrix prescreen gate predicted clinician diagnosis across the ten most common disorders.
Figure 1 presented a cross-diagnostic prediction matrix displaying standardized β coefficients from OLS regression models. Rows represented clinician diagnosis outcomes and columns represented MindMetrix prescreen gates.
The overall multivariate model was significant:
F(10,1051) = 54.976, p < .001
and accounted for substantial variance across all ten diagnostic outcomes:
R² = .02–.30
Gold-bordered diagonal cells represented same-disorder prediction, where a prescreen gate predicted its intended target diagnosis. These were the dominant effects within the model (β = .19–.52), demonstrating discriminant specificity and indicating that each gate most strongly predicted its own intended disorder.
Off-diagonal effects were generally smaller but frequently significant, reflecting the comorbidity structure captured by the prescreen.
Bipolar outcomes reflected Bipolar I Disorder diagnoses.
Key Findings
The analysis included: 1,071 patients with clinician’s ultimate diagnosis recorded in the dataset, drawn from a total of 4,176 MindMetrix assessments.
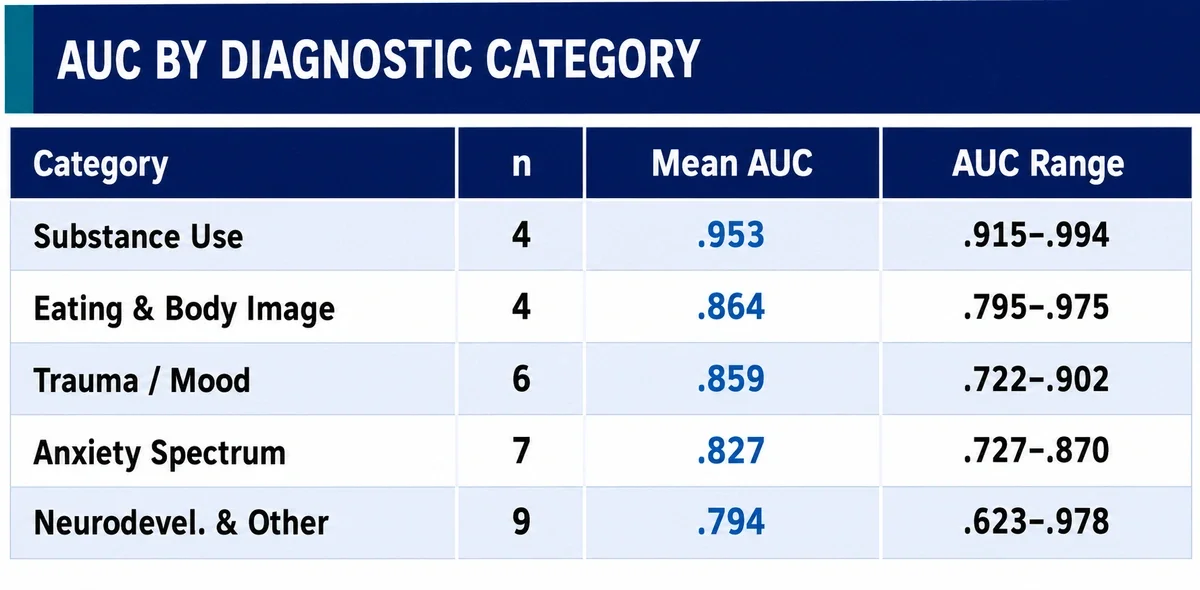
Criterion Validity
- 25 of 30 disorders demonstrated good-to-excellent discrimination (AUC ≥ .80).
- Highest accuracy was observed for low-base-rate conditions:
- Gambling = .994
- Cannabis = .989
- Gender Dysphoria = .978
- Moderate performance for common presentations:
- GAD = .727
- MDD = .722
reflects real-world diagnostic complexity.
- Individual models were significant:
- Nagelkerke R² = .120–.725
- all p < .001.
Internal Consistency
- ICC ranged from .030–.911
- Mean ICC = .453
- SD = .250
- 23 of 26 disorders demonstrated significant reliability (p < .001).
Multivariate Validity
The prescreen significantly predicted clinician diagnoses across the ten most common disorders: F(10) = 54.98, p < .001 despite being designed to guide follow-up testing rather than serve as a standalone diagnostic predictor.
Conclusions
MindMetrix demonstrates strong criterion validity and reliability across a broad range of DSM-5 conditions in outpatient care.
High performance for low-base-rate conditions supports its utility in identifying less commonly considered differentials.
Moderate precision for high-base-rate conditions (ADHD, GAD, MDD) reinforces the role of the full assessment and clinician adjudication.
Future research should validate prescreen performance against clinician rule-outs to support its role in guiding targeted follow-up testing.
Disclosures
Joel L. Young is Co-Founder and Chief Medical Officer of MindMetrix and has received research support from Axsome Therapeutics, Collegium Pharmaceutical, Janssen, Jazz Pharmaceuticals, Lumos Pharma, Supernus, and Tris Pharma, and has served on speakers bureaus and advisory boards for Axsome, Corium, Ironshore, Janssen, Noven, Otsuka, Supernus, and Tris Pharma.
Margot Nash is Co-Founder and CEO of MindMetrix. Jaime Saal is Co-Founder and COO. Ze’ev Lailari serves as CTO. Jill Fortain serves as Director of Test Development.
The study was funded by MindMetrix, LLC.
Ready to boost your practice?
Try 3 complimentary assessments on us.